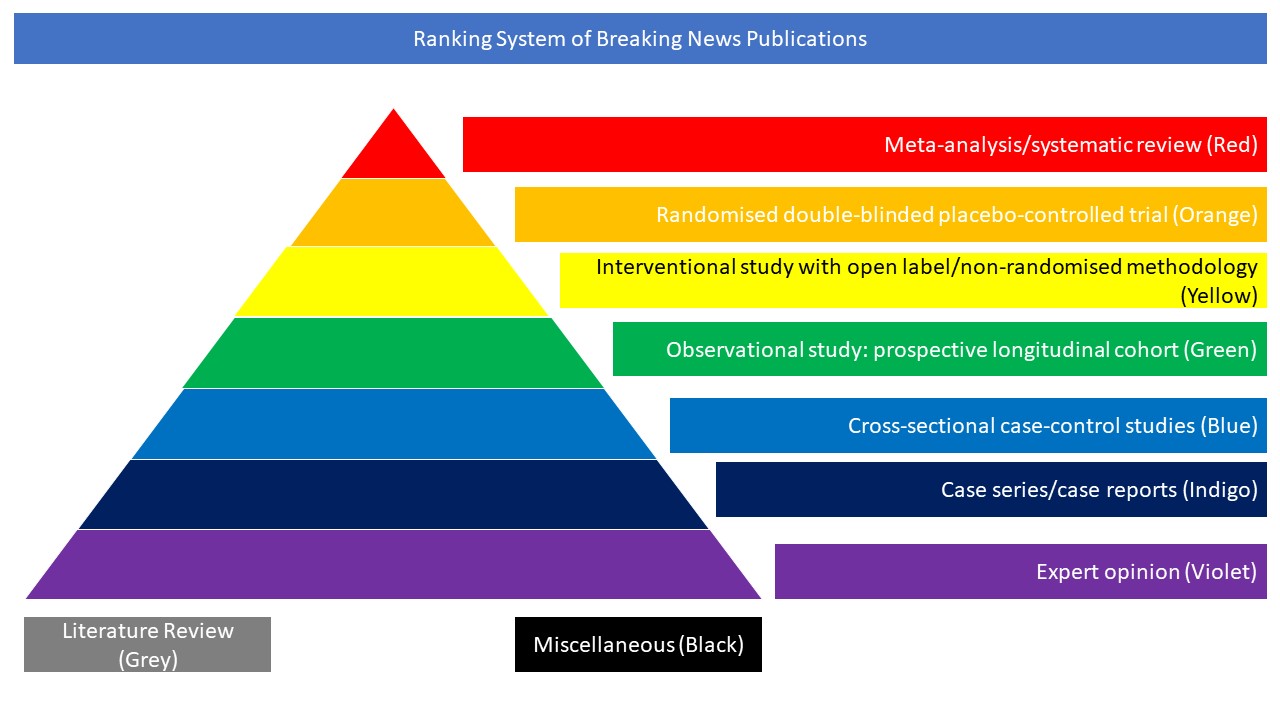
Cross-sectional case-control studies (Blue)
Clinical studies on headache in COVID-19 are limited. This cross-sectional prospective study aimed to define headache characteristics, associated clinical and laboratory factors, and treatment response in COVID-19. 287 patients diagnosed with COVID-19 and hospitalised on a general ward during the pandemic were enrolled. All patients were examined face to face and followed by a neurologist during their stay in the hospital. The characteristics, concomitant symptoms, treatment responses, and laboratory findings of COVID-19-associated headaches were recorded. Eighty-three COVID-19 patients reported headache (28.9%), in which 85.5% had no prior headaches. Mean age was 48.40 ± 15.90 and 58% were men. Compared to COVID-19 patients without headache (n = 204), patients with headache showed significantly higher frequency of pulmonary involvement (76%) and increased D-dimer levels. Fifty-nine percent of headaches responded to iv paracetamol 1000 mg, and 85% of paracetamol unresponsive headaches were relieved by greater occipital nerve (GON) blocks. Latent class cluster analysis identified two distinct classes of bilateral, frontal, throbbing headaches: severe (VAS > 84), longer (> 14 h), frequent (> 7 headache days), paracetamol unresponsive-GON responsive headaches (85%), with pulmonary involvement (100%), and higher IL-6 levels (> 90 pg/mL) were classified in cluster 1. Cluster 2 included moderately affected patients (VAS > 54, > 6 h, > 4 days, 60% pulmonary involvement, > 20 pg/mL IL-6) and paracetamol responsive headaches (96%). VAS scores showed positive linear correlation with IL-6 levels (p < 0.001; r = 0.567). The authors concluded that the intensity, duration, frequency, bilateral frontal location, and treatment response of COVID-19 headache was related to pulmonary involvement and IL-6 levels, which indicated a role of inflammation in determining the headache manifestations in moderately affected hospitalised patients. ROC curve cutoff values pointed that VAS > 70 severity, > 9 h duration, > 5 headache days, and IL-6 > 43 pg/mL levels can be diagnostic for COVID-19 headache. GON blocks can effectively abort headache when patients are unresponsive to paracetamol, and if non-steroidal anti-inflammatory drugs were avoided during SARS-CoV-2 infection.
DOI: 10.1007/s10072-020-04978-2