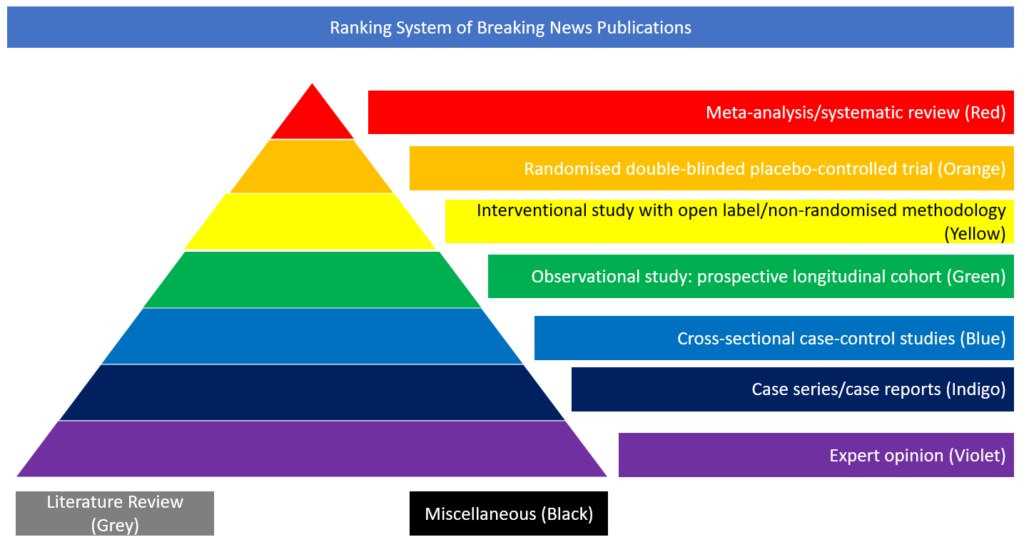
Interventional study with open label/non-randomised methodology
In this controlled, open-label trial recently published in the New England Journal of Medicine, the authors randomly assigned patients who were hospitalised with COVID-19 to receive either oral or intravenous dexamethasone (at a dose of 6 mg once daily) for up to 10 days or usual care.
The primary outcome was 28-day mortality. A total of 2104 patients were assigned to receive dexamethasone and 4321 to receive usual care. Overall, 482 patients (22.9%) in the dexamethasone group and 1110 patients (25.7%) in the usual care group died within 28 days after randomisation (age-adjusted rate ratio, 0.83; 95% confidence interval [CI], 0.75 to 0.93; p<0.001). The proportional and absolute between-group differences in mortality varied considerably according to the level of respiratory support that the patients were receiving at the time of randomisation. In the dexamethasone group, the incidence of death was lower than the usual care group among patients receiving invasive mechanical ventilation (29.3% vs. 41.4%; rate ratio, 0.64; 95% CI, 0.51 to 0.81) and among those receiving oxygen without invasive mechanical ventilation (23.3% vs. 26.2%; rate ratio, 0.82; 95% CI, 0.72 to 0.94) but not among those who were receiving no respiratory support at randomisation (17.8% vs. 14.0%; rate ratio, 1.19; 95% CI, 0.91 to 1.55). In patients hospitalised with COVID-19, the use of dexamethasone resulted in lower 28-day mortality among those who were receiving either invasive mechanical ventilation or oxygen alone at randomisation but not among those receiving no respiratory support.
https://www.nejm.org/doi/full/10.1056/NEJMoa2021436